ACL Reconstruction: Graft Choices

Which graft should I choose for my ACL Reconstruction?
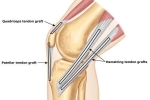
Quadriceps tendon autograft. The quadriceps tendon autograft is often used for primary (initial) reconstruction as well as revision (repeat) reconstruction procedures. The surgeon uses the middle third of the patient's quadriceps tendon with or without a bone plug from the upper end of the kneecap. The size and collagen contact of the graft contribute to its popularity with surgeons and patients.
Potential drawbacks include the following:
- There is a high association with post-operative pain in front of the knee and short delay in quad activation
- Initial post-operative quadriceps muscle spasms
Patellar tendon autograft. A patellar tendon autograft is made up of the middle third of the patient's patellar tendon, along with a bone plug from the shin and the kneecap. It is often recommended for high-demand athletes and patients whose jobs do not require a significant amount of kneeling.
In studies comparing outcomes of patellar tendon and hamstring autograft ACL reconstruction, the rate of graft failure was lower in the patellar tendon group. In addition, most studies show equal or better outcomes in terms of post-operative tests for knee laxity, or looseness, when this graft is compared to others.
The potential drawbacks of the patellar tendon autograft are:
- Post-operative pain behind the kneecap
- Pain with kneeling
- Slightly increased risk of post-operative stiffness
- Slight risk of patella fracture
Hamstring tendon autograft. The hamstring tendon autograft uses the semitendinosus hamstring tendon on the inner side of the knee. Some surgeons use an additional tendon, the gracilis, which is attached below the knee in the same area. This creates a two- or four-strand tendon graft. Hamstring graft supporters claim there are fewer problems associated with harvesting the graft compared to the patellar tendon autograft, including:
- Less anterior (kneecap) knee pain after surgery
- Less postoperative stiffness
- Smaller incision
However, there may be drawbacks to using a hamstring graft, including:
- Post-operative function may be more limited than with the patellar tendon graft
- The size of the patient's hamstring may be less than ideal (diameter)
- The grafts may be slightly more vulnerable to stretching, which can lead to increased laxity (looseness) in the knee
- The patient may have decreased hamstring strength after surgery
Allografts. Grafts taken from human donors are safe, effective choices for certain patients. Allografts are also used for patients who have failed ACL reconstruction, patients ~40 yo or older, or if autograft options have been compromised.
Advantages of using allograft tissue include:
- Elimination of pain caused by obtaining the graft from the patient
- Decreased surgery time
- Smaller incisions
With modern sterilization techniques, the risk of any form of disease transmission from donor to recipient is exceptionally low.
Multiple studies, however, may point to a higher failure rate with the use of allografts for ACL reconstruction. Higher failure rates for allografts have been reported in young, active patients returning to high-demand sporting activities after ACL reconstruction, compared with autografts.
The reason for this higher failure rate is unclear. It could be due to graft material properties (sterilization processes used, graft donor age, storage of the graft). It could also be because the athletes thought the allograft would enable a faster recovery and returned to their sports too soon — before the graft was ready to withstand the loads and stresses of sports. The rate of retear with allografts has not shown to be significantly different in older patients.
Author

Dr. Catherine Logan, MD, MBA
Catherine Logan, MD, MBA, MSPT, is a sports medicine orthopaedic surgeon specializing in complex knee and shoulder surgery at Colorado Sports Medicine and Orthopaedics (COSMO) in Denver, Colorado. As a former physical therapist & trainer, Dr. Logan provides a distinct expertise in sports injury, prevention, and surgical management.